

1/9/23 Edit: So this is explicit, the question deals with the long term. This question is unlikely to resolve within the next few years.
"Significantly" is obviously doing some heavy lifting here. p<.05 isn't going to cut it.
I'm throwing in m500 liquidity to get this started. This might be a perpetual market if there continues to be significant disagreements between reasonable minds. If the odds sit below 2% or above 98% for a significant amount of time then I will resolve the market.
See Isaac King's market on whether COVID-19 came from a lab for equivalent depth of evidence/agreement necessary to resolve, and I will similarly have extensive discussion with bettors prior to any resolution.
 1,000
1,000 3.00
3.00https://www.theepochtimes.com/article/serious-doubt-raised-about-covid-19-vaccine-safety-after-forced-release-of-15000-pages-of-clinical-trial-data-5414614?utm_source=partner&utm_campaign=ZeroHedge&src_src=partner&src_cmp=ZeroHedge

https://www.theepochtimes.com/us/us-military-confirms-myocarditis-spiked-after-covid-vaccine-introduction-5411759?utm_source=partner&utm_campaign=ZeroHedge&src_src=partner&src_cmp=ZeroHedge
https://www.frontiersin.org/articles/10.3389/fcvm.2022.951314/full?trk=public_post_comment-text
[five paragraphs of caveats]
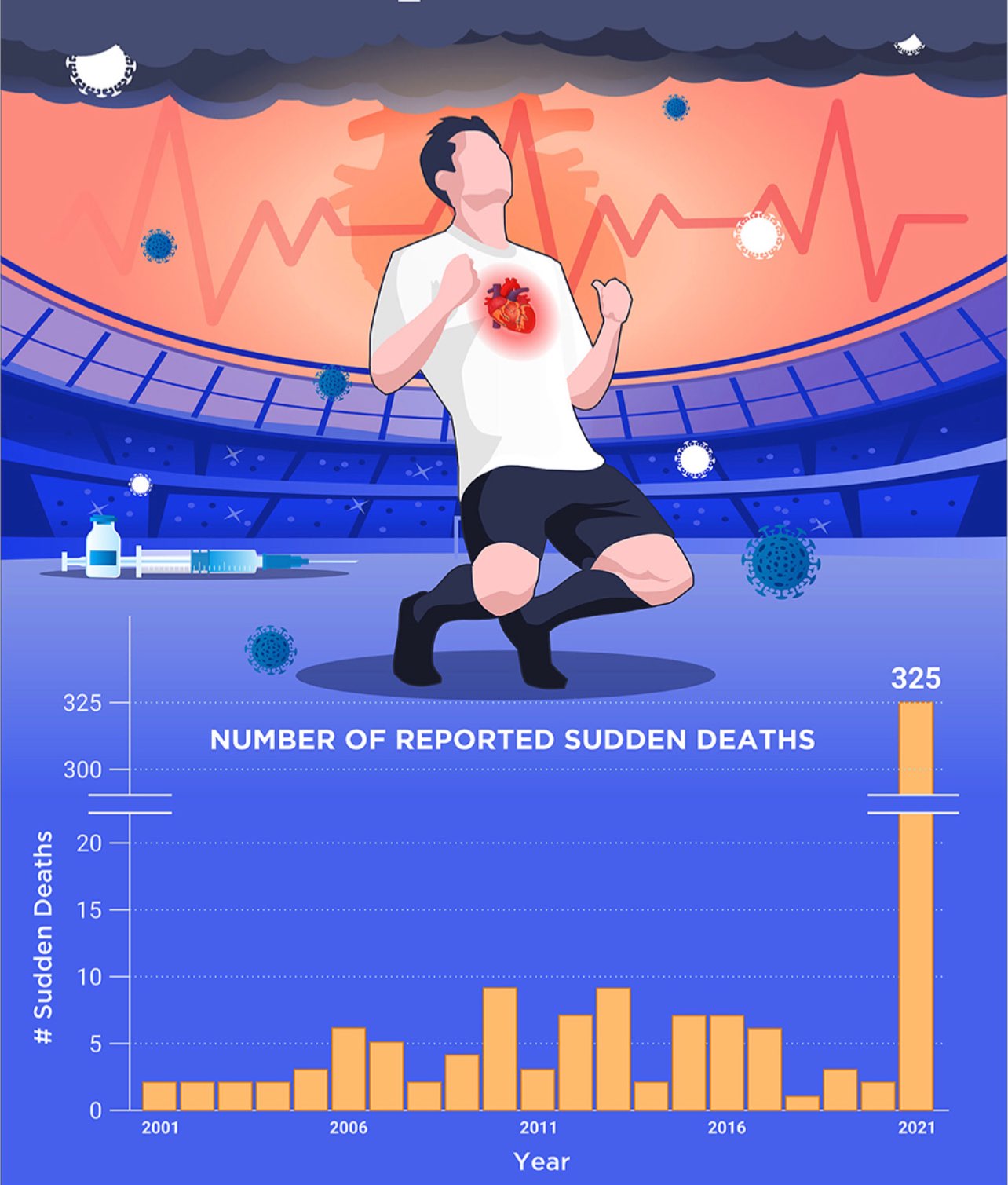
'lots of athletes are dying' is clearly just some bizzare form of media bias. there are not that many athletes. if there was a a noticeable athlete death rate there would be a much more noticeable non-athlete death rate (or the vaccine injuries would somehow be 100x concentrated in athletes) which is weird. much more parsimonious explanation: lots of people who watch lots of media and take it wayyyyy too seriously.

The image posted in the comment seems to come from https://www.frontiersin.org/articles/10.3389/fspor.2022.829093/full, that link to https://goodsciencing.com/covid/athletes-suffer-cardiac-arrest-die-after-covid-shot/
I found two threads talking about this article:
It seems to be a case of base rate error and using different criteria between years.
An effect size threshold would be nice. In observational studies, I’d feel safe betting on any comparison getting some p-value “stars” as N goes into millions because, without ideal experimental randomization, even small coincidences get to bite us stronger and stronger instead of washing out more and more.
The two official, worldwide, randomized and observer-blinded trials are the obvious first go-to. Epidemiological studies may in theory be able to pick up smaller effects (thanks to larger samples) but this is dwarfed by them having way more confounds and colliders. If there was an effect, it would seem to be too small to be reliably detected by either.
“Adverse event analyses are provided for all enrolled 43,252 participants (…). Two BNT162b2 recipients died (one from arteriosclerosis, one from cardiac arrest), as did four placebo recipients (two from unknown causes, one from hemorrhagic stroke, and one from myocardial infarction). No deaths were considered by the investigators to be related to the vaccine or placebo.” (https://www.nejm.org/doi/full/10.1056/nejmoa2034577)
“30,420 participants underwent randomization, and the 15,210 participants in each group were assigned to receive two doses of either placebo or mRNA-1273 (…). Three deaths occurred in the placebo group (one from intraabdominal perforation, one from cardiopulmonary arrest, and one from severe systemic inflammatory syndrome in a participant with chronic lymphocytic leukemia and diffuse bullous rash) and two in the vaccine group (one from cardiopulmonary arrest and one by suicide).” (https://www.nejm.org/doi/full/10.1056/nejmoa2035389)
@yaboi69 I'm open to suggestions on how to assess a significant effect size.
This question is also addressing long term effects though, so any "no" resolution will need to wait some time.
@NickAllen Given the clear demographic differences between those who do/don't take the mRNA vaccine (most obviously age, nationality, ethnicity), and the many other factors that would have to be adjusted for (with some difficulty!), are you likely to accept observational evidence alone in resolving 'yes'? Or would you require experimental studies like those linked above, whether new or follow-up?
@NickAllen We’re likely to get more phase 2/3 experiments as researchers propose more mRNA treatments in other groups and for other diseases like cancer. This will provide some more relatively high-quality randomized comparisons. We also need and have theoretical work and in vitro studies to inform us. But then, in practice, there’s also a whole other dynamic at work. If a risk factor is identified or suspected, public health institutions and doctors are going to adjust their behaviors accordingly.
This gets us to another important question. What is the actual comparison (what is the counterfactual)? The “all-cause mortality” wording refers to a well-known demographic indicator for real populations. In the real world population with the presence of COVID and cancer, and where vaccine use is non-random, a reduction in these diseases would outweigh on net even wildly high adverse event levels. So is it enough if the trials basically ruled out adverse event risk levels that would be higher than disease risk levels (they did that and more, in all age groups)?
@WXTJ I'll consider both observational and experimental. Given how broad the available data is, and how the factors determining vaccination changed from country to country I think observational studies shouldn't be ruled out.
@yaboi69 they'd need to do that for an extended period of time. The question isn't just about the first few weeks after vaccination. I expect this question to be open for several years at least, until the politics have cooled down and the effects have gotten to the steady state.
@jacksonpolack yes I wonder if this market was made with the premise that 'all-cause mortality' would not include death attributed to SARS-2 CoV. That wasn't set out in the market though, so I think they should definitely require evidence of a
net increase in all-cause mortality with COVID deaths included.
What hasn't been clarified is if this is all-cause mortality at a population level, or if they would include narrower samples, eg a young age group, or an immunocompromised group. Would, for instance, convincing evidence that a single narrow group in one country had a net increase in all-cause mortality be adequate to resolve yes?
@jacksonpolack the normal course of novel coronaviruses has an decrease in the death rate over time, so the amount that the vaccines help will decrease as well, and if the long term harm starts to outweigh the benefit then that would be one situation this question will look at.
Additionally, virologists recommend against deploying leaky vaccines against fast-mutating viruses like COVID-19 because it ends up changing the selection pressures and actually increasing lethality in the long term, which is another factor we'll be keeping an eye on.
the normal course of novel coronaviruses has an decrease in the death rate over time, so the amount that the vaccines help will decrease as well, and if the long term harm starts to outweigh the benefit
this is not happening, because the death rate among oldish people was quite high initially, and booster uptake rates are very low. even if the boosters were a bit bad, not enough people are taking them
Additionally, virologists recommend against deploying leaky vaccines against fast-mutating viruses like COVID-19
explain how this is different than the flu vaccines